On November 29, 2017, the results of two studies on the efficacy of antibodies against CGRP for the prevention of chronic and episodic migraine, respectively, were published in the New England Journal of Medicine.<sup> 1,2</sup> Antibody therapy targets a molecule that plays a key role specifically in inflammation, sensitization, and pain during a migraine attack. The current facts are summarized below.
Current facts about migraines
- Migraine is the third most common disease worldwide (after tooth decay and tension headaches), with an estimated global one-year prevalence of 14.7%. This means that approximately one in seven people suffers from migraine attacks within a year. Nearly one in three women between the ages of 30 and 40 are affected.
- Migraines are more common than diabetes, epilepsy, and asthma combined.
- Chronic migraine affects approximately 2% of the world's population. The World Health Organization (WHO) estimates that between 127 and 300 million people worldwide suffer from chronic migraine.
- Migraines affect three times as many women as men.
- Every day, 900,000 people in Germany are affected. 100,000 people are unable to work and bedridden each day due to migraines.
- On average, 8.3 million Germans take a headache tablet every day through self-medication.
- An average of 58,853 single doses of triptans, which are special migraine medications for treating attacks, are taken every day in Germany
- More than half of those affected experience severe impairment as a result of the seizures.
- Migraines often begin in puberty. They are most debilitating between the ages of 35 and 45. However, many young children are also affected. In recent years, there has been a significant increase, particularly among children.
- Migraine ranks seventh worldwide among the most debilitating diseases and is the leading cause of disability among all neurological diseases.
- It is estimated that the German population loses 32 million working days due to migraines.
- Severe migraine attacks are classified by the World Health Organization as among the most disabling diseases, comparable to dementia, paraplegia affecting all four limbs (legs and arms), and active psychosis.
- Migraines and chronic headaches are the second most common reason for short-term incapacity for work.
- In Germany, sick leave due to migraine alone costs 3.1 billion euros per year, calculated on the basis of 32 million lost days.
- The risk of depression, anxiety disorders and suicide is 3 to 7 times higher in affected individuals than in healthy individuals.
- The risk of cardiovascular disease, heart attack, and stroke is 1.5 to 2 times higher than in healthy individuals. This is especially true for young women under 45.
- It is scientifically established that migraines have a genetic basis. Currently, 44 gene variants on 38 risk genes for migraines are known.
- One of the most common health problems treated with scientifically unproven, unconventional therapies is headache.
- Worldwide, on average, only about two to four hours are dedicated to information on headache diagnosis and treatment during the six-year medical degree program.
- Despite the proven effectiveness of using specialist nurses for headache treatment, there is no specialized training in Germany.
- Migraine and other headaches were first classified internationally in 1988 by the International Headache Society (IHS), which also described operationalized diagnostic criteria. The International Classification of Headache Disorders, 3rd Edition (ICHD-3) beta, was published in 2013 and is recognized by the World Health Organization. Researchers and clinicians worldwide refer to these internationally valid diagnostic criteria. Currently, 367 principal diagnoses of headaches are distinguished. No other neurological disorder has a comparable, differentiated diagnostic and classification system.
The facts about the development of migraines
Today, it is known that migraine patients exhibit numerous genetic peculiarities. Currently, 38 gene loci with 44 gene variants are known to increase the risk of developing migraines. These gene variants control, on the one hand, nerve impulse transmission, sensitivity, and processing. On the other hand, they also regulate the energy supply to nerve cells and the regulation of arterial walls. Arterial walls should not be imagined as lifeless tubes. Rather, the lining of blood vessels is the largest endocrine organ in our body. Numerous messenger substances are produced here that regulate blood flow and inflammatory responses. Many substances relevant to important regulatory processes in our body are also activated here. A disruption in energy supply, for example, due to oxidative stress, can throw this regulation off balance and lead to malfunctions. Thus, genetic predisposition, as well as environmental, behavioral, and social factors, play a significant role in the development of migraine attacks.
The unique characteristics of migraine predisposition mean that sufferers can perceive stimuli very intensely. They are also able to actively and precisely differentiate between stimuli. If stimuli occur repeatedly, migraine patients do not become accustomed to them, but rather can perceive them with great nuance; so-called stimulus adaptation and distraction from stimuli hardly occur. As a result, migraine patients, figuratively speaking, can hear the tap dripping three rooms away. They already have answers to questions that no one has even asked yet. They color their thoughts and perceptions with emotions much more intensely. They perceive changes in their environment very quickly; for example, if a picture is hanging crooked on the wall, they notice this immediately and feel the impulse to straighten it. This rapid and active processing of stimuli can also lead to very significant achievements. Many famous people who have accomplished great things also suffered from migraines. Examples include Marie Curie, who suffered from severe migraine attacks almost daily as a student and later became the only person to receive a Nobel Prize in two different scientific fields. Richard Wagner, in the opening bar of his opera "Siegfried," musically depicted his own migraine, translating the pulsating and throbbing headache into sound and even creating a musical monument to his visual migraine aura. Vincent van Gogh also captured on canvas how seeing during a visual aura alters perception. Other examples include Charles Darwin, Alfred Nobel, Salvador Dalí, Claude Debussy, Frédéric Chopin, and many more. It is important to manage this particular "operating system" in such a way that one's behavior and lifestyle allow for the smoothest possible functioning. The most important rule is regularity and consistency, so that anything too fast, too many, too sudden, or too impulsive in daily life can be avoided, thus preventing sensory overload and the depletion of neural energy.
Facts about CGRP
For the first time, researchers have succeeded in developing specific antibodies against messenger substances that cause inflammation in the arteries of the meninges. Administering so-called monoclonal antibodies can halt the effects of these inflammatory substances for several weeks and significantly reduce the likelihood of migraine attacks. The inflammatory protein CGRP plays a central role in this process. Currently, four antibodies targeting this protein are being developed and tested in numerous studies.
The antibodies currently available have all demonstrated their efficacy in very large-scale international studies. Some antibodies act directly against CGRP, while others block the CGRP receptor. They must be administered approximately four weeks apart.

The antibody (blue) blocks the CGRP receptor (orange) and protects it from CGRP. CGRP can no longer reach and activate the receptor, thus preventing inflammation and pain.
Unlike all other currently available preventative medications, this new immunotherapy is the first to be specifically developed for migraine prevention. A slow dose titration due to intolerances and side effects is not necessary. The onset of action is rapid, initially within a few days, whereas with conventional preventative medications, this often takes weeks or even months. Side effects of previous migraine preventatives, such as weight gain, mood swings, fatigue, reduced energy, or drowsiness, do not occur. In contrast to previous medications, which are frequently discontinued after a short time due to such side effects, patients treated with this approach remain on it long-term due to its tolerability and efficacy.
Fremanezumab reduces migraine frequency in phase 3 study in chronic migraine
Prophylactic administration of fremanezumab significantly reduces the number of headache days per month in patients suffering from chronic migraine. The drug can be administered every one or three months. Clinical efficacy was confirmed in a phase 3 study published 29
The study included 1,130 patients suffering from chronic migraine. Chronic migraine is characterized by headaches occurring on more than 15 days per month, with at least 8 of those days corresponding to the typical pattern of migraine attacks. The patients were randomly assigned to three equally sized groups. The first group received a single dose of 675 mg fremanezumab at the start of treatment, followed by injections of a placebo at 4 and 8 weeks. The second group received 675 mg fremanezumab at the start of treatment, followed by injections of 225 mg fremanezumab at 4 and 8 weeks. The third group received a placebo at each of the respective time points.
After 12 weeks, the reduction in headache days per month by at least 50% was assessed. The percentage of patients who achieved this reduction of at least 50% in their attack frequency was:
- 38% in the group that received fremanezumab quarterly
- 41% in the group that received fremanezumab with monthly treatment and
- 18% in the placebo group.
Placebo was significantly less effective in both groups (P < 0.001).

Adverse events were reported in 64% of patients receiving placebo, 70% of patients receiving fremanezumab every three months, and 71% of patients receiving fremanezumab every month. These adverse events were of mild to moderate intensity in 95–96% of patients across all three groups. The most common adverse event was injection site pain, occurring in 30% of patients receiving fremanezumab every three months, 26% receiving it every month, and 28% receiving placebo. Adverse events led to study discontinuation in 1% of patients in the quarterly group, 2% in the monthly group, and 2% in the placebo group.
Patients can continue treatment with the antibody after completion of the double-blind study to analyze its efficacy and safety over long-term use. The study results are consistent with previous dose-finding studies in chronic migraine. The authors state that further studies are needed in patients with migraine and its common comorbidities.
Erenumab shows a reduction in attacks in a phase 3 study in episodic migraine.
In the same issue of the New England Journal of Medicine on November 29, 2017, new data on erenumab in the prevention of episodic migraine were also published. Erenumab was administered subcutaneously every four weeks at a dose of 70 mg or 41 mg. The analysis showed that the antibody significantly reduced migraine frequency, the impact of migraine on daily activities, and the need for acute migraine medication over a six-month period.
The study included 955 patients. 317 received erenumab 70 mg, 319 received erenumab 140 mg, and the remaining 319 patients received a placebo. At the start of the study, the mean frequency of migraine days per month was 8.3.
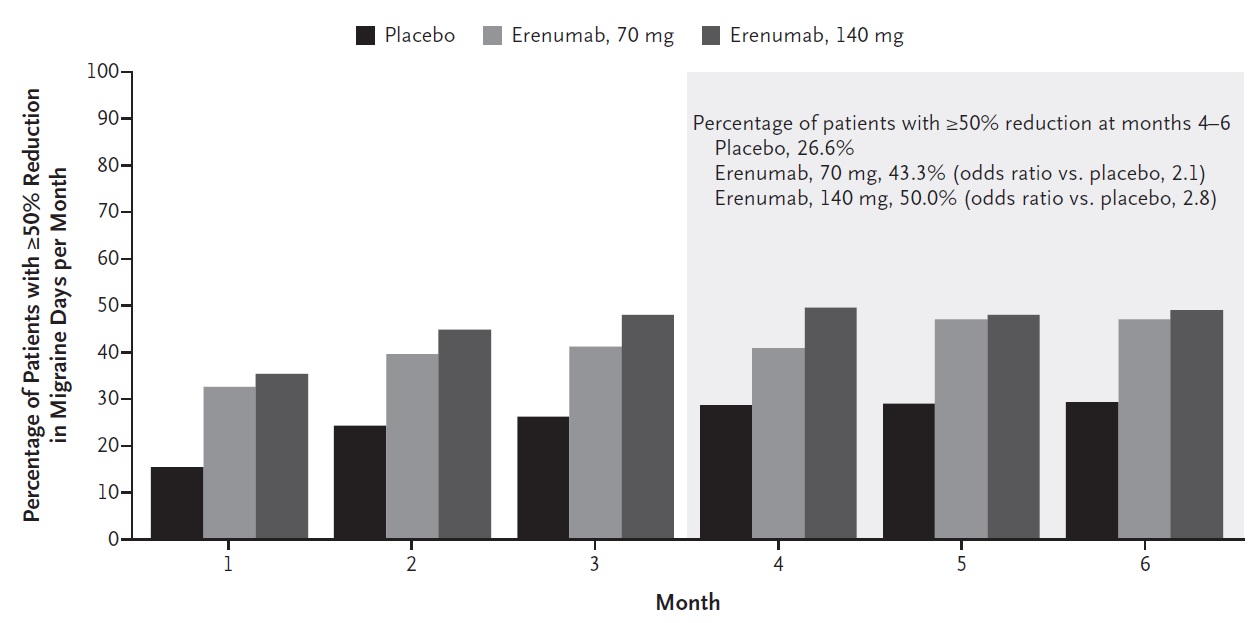
Rate of at least 50% reduction in migraine days per month compared before treatment with the frequency during the double-blind treatment phase (2)
The efficacy parameters were analyzed after 4-6 months of treatment. The following results were obtained:
The number of migraine days was reduced by
- 3.2 days in the 70 mg erenumab group
- 3.7 days in the 140 mg erenumab group
- 1.8 days in the placebo group (P < 0.001 for each dose versus placebo)
A reduction of more than 50% in the average number of migraine days per month was achieved for
- 43.3% of patients in the 70 mg erenumab group
- 50% of patients in the 140 mg erenumab group
- 26.6% in the placebo group (P < 0.001 for each dose versus placebo)
The number of days requiring the use of acute migraine medication has been reduced to
- 1.1 days in the 70 mg erenumab group
- 1.6 days in the 140 mg erenumab group
- 0.2 days in the placebo group (P < 0.001 for each dose versus placebo)
The physical disability improved by the following scores:
- 4.2 points in the 70 mg erenumab group
- 4.8 points in the 140 mg erenumab group
- 2.4 points in the placebo group (P < 0.001 for each dose versus placebo)
Daily activities improved by the following percentages, as measured by the analyzed scores:
- 5.5 points in the 70 mg erenumab group
- 5.9 points in the 140 mg erenumab group
- 3.3 points in the placebo group (P < 0.001 for each dose compared to placebo)
The frequency and severity of adverse events were approximately the same in the groups receiving erenumab and those receiving placebo.
The authors conclude from these data that erenumab may be an effective substance in the prevention of episodic migraine. Further studies are needed to analyze its long-term safety and tolerability. The long-term efficacy and the sustainability of clinical effects also require further investigation in additional studies.
And what do the results mean for healthcare provision?
Extensive analyses show that the new substances only have a clinical effect in a subset of patients. Looking at the mean reduction in headache days per month, the changes compared to placebo are significant, but clinically similar to those of existing preventive medications. Migraine attacks may still occur.
Their frequency can be reduced by an average of about 25% compared to a placebo. However, there are also patients who respond very well to the treatment and whose headaches almost completely disappear. This effect can be explained by the fact that CGRP is only one of several neurotransmitters that play a significant role in the development of migraines.
This is to be expected. If at least 38 risk genes and 44 gene variants are responsible for the various mechanisms involved in migraine, a complex basis exists with diverse pathways in the nervous system to generate migraine attacks. Patients in whom CGRP plays a central role can expect significant relief with appropriate treatment.
Other affected individuals, in whom other mechanisms are the primary focus, must wait for future therapeutic developments.
However, these new substances offer, for the first time in human history, a specific way to prevent migraines by directly intervening in their underlying mechanisms. While previous migraine medications only demonstrated their effectiveness incidentally when used to treat other diseases, the new antibodies were specifically developed for migraine prevention. They offer new hope for patients who have not previously received adequate relief. A further advantage is that the new antibodies act outside the blood-brain barrier, thus avoiding central nervous system side effects such as fatigue, dizziness, mood swings, and weight gain.
While some patients experienced a 100% reduction in attack frequency, others did not respond to the treatment. The degree of effectiveness varied considerably among the treated study participants.
The new findings show that a new door has been opened in the treatment of migraines. Should the current data be confirmed, more patients will be able to reduce their migraine burden and return to a normal life in the future.
The desire to eliminate attacks without adapting one's life to a migraine predisposition can also be dangerous. The dream of disregarding the most important preventative rule—namely, maintaining regularity and a consistent rhythm—in order to simply live life to the fullest, can become a problem. Anything too fast, too numerous, too sudden, or too impulsive then leads to sensory overload and depletion of neural energy. In the long run, this can cause psychological and physical complications. Complex underlying mechanisms therefore continue to require comprehensive treatment.
It's like a flat bicycle tire with five holes. If you only patch one, the air will be out again the next morning. You have to find all five leaks and patch them at the same time before you can ride.
literature
1 Silberstein SD, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med 2017;377:2112-22. http://www.nejm.org/doi/full/10.1056/NEJMoa1709038
2 Goadsby PJ, et al. A controlled trial of erenumab for episodic migraine. N Eng J Med 2017;377:2123-32. http://www.nejm.org/doi/full/10.1056/NEJMoa1705848





Thank you so much for these very informative posts. I can completely understand all migraine sufferers, as I've been suffering from them myself for 53 years. I've tried just about everything, but with little success. I sincerely hope that this new medication will be officially approved in Germany as soon as possible and thus be available to everyone. Coverage of the costs by health insurance companies would also be very welcome!
Marlene Kempel:
My biggest worry is that I won't be able to take triptans anymore because I suffer from coronary artery disease. At the moment, I'm just continuing to take them since regular painkillers, even high doses, don't help. I'm constantly looking for alternatives, but so far I haven't found anything that can permanently and effectively reduce the pain. By now I could write a book about all the attempts I've made. Aside from the immense costs, which I've often had to bear myself, the disappointment is huge when there's no improvement whatsoever.
I've also suffered from migraines for 30 years and am very happy about the progress in medicine. Hopefully, this medication will be available soon. I've been on disability pension for four years now because of my migraines.
A glimmer of hope in the complex chaos of migraines; we can only thank the people who are researching this scourge of migraines so intensively.
But how does one get involved in a study or receive treatment?
In any case, I am very pleased with this excellent article.
Olaf Biewald
I, Monika Kornberger, was an inpatient at the Kiel Pain Clinic in 2014. I have suffered from migraines since I was 27. I am now 65 and
still have severe migraines. I don't have a single pain-free day. I have recently been diagnosed with trigeminal neuralgia, primarily on the right side and beginning to affect the left. I have
n't given up hope for improvement. I have very severe headaches, accompanied by tinnitus. I also have balance problems.
Because of the pain, I don't socialize as much anymore. I would be very grateful if this new medication would help.
Thank you for the detailed and, above all, understandable explanation of the CGRP development in this December 2017 newsletter. Appropriately for Christmas: The big door of the advent calendar is about to open. While anticipation isn't exactly the greatest, hope for a positive effect is spreading, and that's something.
Merry Christmas and a hopeful 2018.
Thank you so much for the clear explanation of the effects of migraines. I've never read or heard such a description before. It makes me feel truly understood and taken seriously. It would be wonderful if the description above – "Severe migraine attacks are classified by the World Health Organization as one of the most disabling diseases, comparable to dementia, paraplegia affecting all four limbs (legs and arms), and active psychosis" – had a corresponding impact on disability assessments, pension applications, and so on. And it would be even better if one of the new medications could help me. Thank you for your work.
That gives me hope. I hope that antibody treatment can be used given my medical history. Relief after 39 years of migraines!?
Very hopeful. It would be highly desirable to have such a medication available. A new life for me after 43 years of migraines.