



The first week of September is used internationally to raise awareness about migraines and highlight the significant impact of this health problem. The aim is to reduce prejudice and stigma. Professor Hartmut Göbel answers current questions about migraines, their effects, and treatment
What significance do migraines and headaches hold for society?
Representative studies show that 71% of Germans report suffering from headaches at some point in their lives. This figure includes all 367 known types of headaches. In Germany, this means that approximately 54 million people suffer from recurring headaches. Headaches can persist for extended periods, often spanning 40 to 60 years. They cause significant suffering and considerably impair quality of life and ability to work. The World Health Organization ranks migraine as the seventh most disabling disease. Considering all types of headaches together, they rank third among the most disabling diseases.
Migraines have existed since the dawn of humankind. The first severe migraine attack is described in great detail on an Egyptian papyrus. Migraine attacks are repeatedly documented in world literature. Even the Apostle Paul's Damascus experience, with its visions of light and three days of bedridden illness with loss of appetite, demonstrates that migraines are not a modern phenomenon, but have existed since time immemorial.
And here are some important facts:
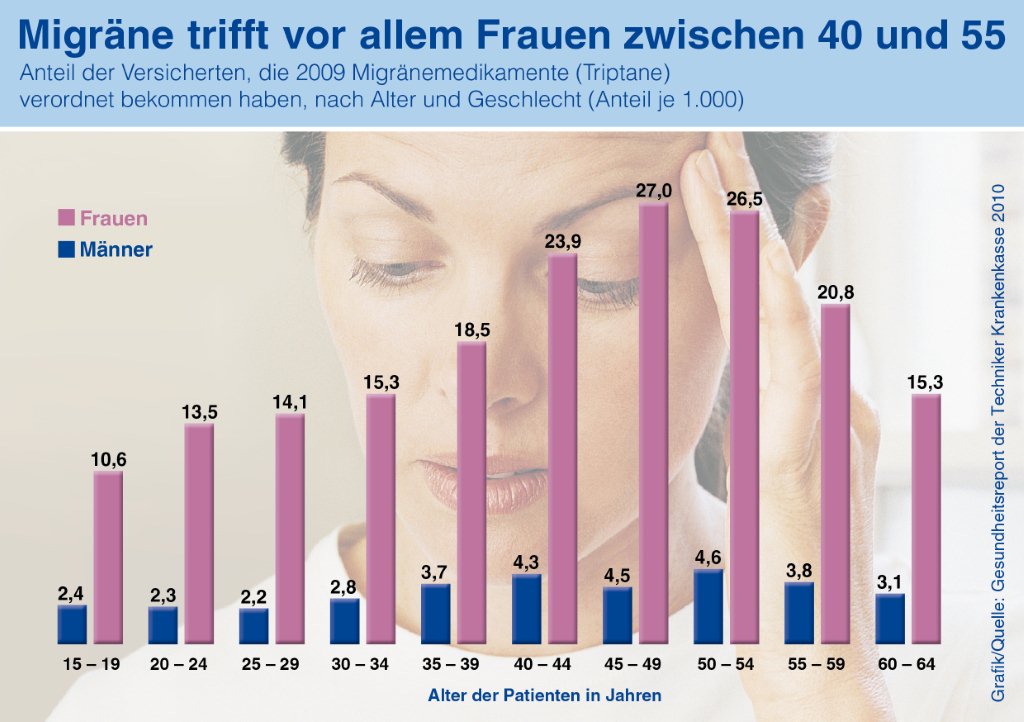
- Migraine is the third most common disease worldwide (after dental caries and tension headaches), with an estimated global one-year prevalence of 14.7% (i.e., about one in seven people). Nearly one in three women between the ages of 30 and 40 are affected.
- Migraine is more common than diabetes, epilepsy and asthma combined.
- Chronic migraine affects approximately 2% of the world's population.
- Migraines affect three times as many women as men.
- 900,000 people in Germany are affected every day. 100,000 people are unable to work and bedridden every day because of migraines.
- On average, 8.3 million Germans take a headache tablet every day through self-medication.
- On average, 58,853 individual doses of triptan, which are special migraine medications for treating migraines, are taken every day in Germany
- More than half of those affected experience severe impairment as a result of the attacks.
- Migraines often begin during puberty. It is most disabling between the ages of 35 and 45. But many young children are also affected. In recent years there has been a strong increase, particularly among children.
- Migraine is the seventh most debilitating disease worldwide and the leading cause of disability among all neurological diseases.
- It is estimated that the German population loses 32 million working days due to migraines.
- Severe migraine attacks are classified by the World Health Organization as among the most disabling diseases, comparable to dementia, paraplegia affecting all four limbs (i.e., both legs and arms), and active psychosis.
- Migraines and chronic headaches are the second most common reason for short-term incapacity to work.
- Incapacity to work due to migraines alone costs 3.1 billion euros per year in Germany, calculated based on 32 million days lost.
- The risk of depression, anxiety disorders and suicide is 3 to 7 times higher in affected individuals than in healthy individuals.
- The risk of cardiovascular disease, heart attack, and stroke is 1.5 to 2 times higher than in healthy individuals. This is especially true for young women under 45.
- It is scientifically established that migraines have a genetic basis. Currently, 44 gene variants on 38 risk genes for migraines are known.
- One of the most common health problems treated with scientifically unproven, unconventional therapies is headache.
- Worldwide, on average only about two to four hours of information about headache diagnosis and treatment are offered during the six-year medical course.
- Despite the proven effectiveness of using specialist nurses for headache treatment, there is currently no specialized training in Germany.
- Migraine and other headaches were first classified internationally in 1988 by the International Headache Society (IHS), which also described operationalized diagnostic criteria. The International Classification of Headache Disorders, 3rd Edition (ICHD-3) beta, was published in 2013 and is recognized by the World Health Organization. Researchers and clinicians worldwide refer to these internationally valid diagnostic criteria. Currently, 367 principal diagnoses of headaches are distinguished. No other neurological disorder has a comparable, differentiated diagnostic and classification system.
Is migraine sometimes still seen as an excuse?
Unfortunately, this situation is characterized by either complete ignorance or, at worst, malicious intent. Discrimination against people because of a disability or their genetic makeup should be a thing of the past. Migraine is a biological disease. The World Health Organization considers it one of the most debilitating diseases in humans. Currently, 44 gene variants have been identified, linking 38 risk genes and demonstrating that our body's blueprint contains biological factors that contribute to the risk of developing migraine. Migraine is a serious disorder of the nervous system that causes significant individual suffering and severely disables those affected.
Should more information be provided about migraines and headaches?
Many people who suffer from headaches don't have a specific diagnosis. Only about a third have a name for their headaches. Currently, over 367 different types of headaches are recognized internationally. Most of these aren't even known by name in standard medical care. Specific treatment options aren't offered to those affected. Patients themselves often lack an understanding of the cause of their headaches or how to treat them effectively. Therefore, it is crucial that specific treatment pathways are made available to those affected.
How can you recognize migraines and tension headaches?
Migraine attacks are episodic headaches lasting from 4 to 72 hours. The headache is characterized by a throbbing, pulsating pain. It is felt in a specific area of the head. Physical activity intensifies the pain, which is often very severe, severely hindering or even preventing activity. The pain may be accompanied by nausea, vomiting, and sensitivity to noise and light. In contrast, tension-type headaches present as a dull, pressing, bilateral headache. Physical activity does not intensify the pain, and nausea and vomiting are not present.
Are women more frequently affected?
According to representative studies, women suffer from migraines approximately two to three times more often than men. Scientific studies indicate that faster, more active processing of stimuli in the central nervous system is responsible for this.
Why do some people get migraines while others don't?
Recent studies have shown that specific risk genes increase the likelihood of developing migraines. In the world's most comprehensive migraine study to date, 44 new gene variants were discovered. These variants are associated with an increased risk of migraine. Many of these gene variants are located in the regions of the genome that regulate the brain's circulatory system. These new discoveries indicate that a disruption in the brain's blood and energy supply is essential for the development of migraines. They represent a milestone in understanding the causes of migraines.
How does migraine behave across the lifespan?
Migraine attacks typically begin around age 7. By age 14, more than 14% of girls and more than 7% of boys are affected. The peak incidence of migraines occurs in the third and fourth decades of life.
Which doctor should I consult for migraines and headaches?
Migraine is a neurological disorder of the central nervous system. If left untreated, it can lead to serious complications. In addition to psychological complications, serious physical illnesses can also occur if migraine is not effectively treated. These include an increased risk of stroke, heart attack, and other cardiovascular diseases. The opinion still persists in some quarters that this serious condition should be treated with unconventional or alternative therapies. However, based on current scientific knowledge, there is definitely no place for this. Migraine must be treated as effectively as possible to prevent it from becoming chronic and to avoid serious long-term complications. The first point of contact is the general practitioner. In complex cases, a neurologist is consulted as a specialist, and for severe cases, a pain specialist is also the appropriate contact person.
What happens in the brain?
In principle, migraine is not caused by any structural disorder in the brain; the brain's structure is normal. However, due to their genetic makeup, migraine sufferers can differentiate stimuli very quickly and effectively. Anything too fast, too numerous, or too sudden—anything that floods the nervous system all at once—leads to a strong activation of nerve cells, resulting in the depletion of their energy reserves. This repeatedly leads to a disruption in the regulation of nerve function, which can then break down, triggering a migraine attack.
If such a malfunction of nerve function occurs, inflammatory substances can be released from the arteries of the meninges. These lead to increased sensitivity of the meninges. Every heartbeat results in a throbbing, pounding migraine pain; every movement of the head hurts. Therefore, migraine sufferers try to rest as much as possible and avoid physical activity. Migraine pain is thus based on neurogenic inflammation with heightened pain sensitivity.
What triggers seizures?
The most important factor triggering migraine attacks is irregularity in daily life and excessive energy demands on nerve cells. Stress, irregularity, everything too fast, everything too much, everything too sudden, everything at once, can trigger migraine attacks.
How are migraines treated today?
Modern migraine therapy rests on three crucial pillars. The first pillar consists of knowledge and information. Migraine patients need to understand how migraine attacks develop, what happens in the nervous system, and what triggers them. They need comprehensive information about behaviors and measures to protect themselves from migraines. This primarily includes a regular day-night rhythm. Patients should eat regular meals. Carbohydrate-rich meals are recommended, as the nervous system relies on carbohydrates. Migraine attacks arise from an energy deficit in nerve cells due to their genetically determined high activity. Adequate hydration, regular sleep, and regular breaks throughout the day should also be implemented. Learning a relaxation technique such as progressive muscle relaxation can significantly reduce the frequency of migraines. Information from patient guides or online resources can also provide a wealth of knowledge that helps reduce migraine frequency in everyday life. Self-help groups, such as... The online platform www.headbook.me, for example, can facilitate exchange and share knowledge with those affected. Exercise therapy is also well-suited to reducing the frequency of migraine attacks. Regular endurance exercise such as running, swimming, or cycling is particularly helpful. If there are more than seven headache days per month, medication prophylaxis should be considered in addition to the measures described. This consists of various medication options and includes beta-blockers, calcium channel blockers, antiepileptics, antidepressants, and other substances. The choice of medication should be individualized and must be discussed with a doctor. Several options exist for treating an acute attack. For mild attacks, pain relievers such as aspirin, ibuprofen, or paracetamol can be used. If nausea and vomiting occur, antiemetics such as metoclopramide are administered. For severe attacks, seven different triptans are available in various formulations. In cases of severe nausea or vomiting, the active ingredient can also be self-injected subcutaneously using a pen; it is also available as a nasal spray. Triptans should be taken as early as possible during an attack, and the 10-20 rule applies here as well. They should be used on fewer than 10 days per month to avoid medication overuse headache (MOH). Newer treatment options for chronic migraine, i.e., migraine that occurs more than 14 days per month, include botulinum toxin and neuromodulation. These can be used by specialized headache centers in particularly severe cases.
What mistakes can you make?
The most common mistake is failing to implement information on behavior, prevention, and other preventative measures. This quickly leads to a rapid increase in attacks, resulting in the overuse of acute medications. Taking acute medications on at least ten days a month alters the sensitivity of the nervous system. This leads to increased sensitization and the development of medication-overuse headache. A cycle of increasingly frequent attacks ensues, necessitating ever more frequent use of acute medications, until eventually chronic headache develops. Therefore, the most important rule is: acute headache medications should be taken on fewer than 10 days per month. At least 20 days per month should be free of acute medications for treating headache attacks.
Do you have to accept migraines?
You can't simply accept pain and migraines. You don't get used to pain. On the contrary, pain breeds more pain. Enduring pain is not a virtue. You have to actively treat it. With today's therapeutic options, there are very effective and well-tolerated treatment strategies for managing headaches. However, you have to become your own advocate, take the initiative, gather knowledge and information, and then implement targeted preventative measures.
How do you proceed with treatment at the Kiel Pain Clinic?
Our treatment concept focuses on neurological pain disorders such as migraines, chronic headaches, and other pain conditions associated with diseases of the nervous system. These are among the most debilitating conditions and, after dementia and stroke, among the three most expensive neurological diseases. Traditional sectoral boundaries in care and medical specialties exacerbate their tendency to become chronic. At its core is multimodal pain therapy, meaning the consistent, interdisciplinary application of international scientific knowledge to the needs of patients, indication-specific collaboration among specialized practitioners, and networking. The goal is to sustainably alleviate pain, restore quality of life, and enable patients to return to work. The clinic has received numerous awards for its innovative treatment concept, including the prize for the best implementation of integrated care in Germany. Patient satisfaction within the nationwide treatment network is very high. This is repeatedly confirmed by both patients and health insurance companies.
What advice do you give to family members?
Relatives of migraine sufferers should also thoroughly inform themselves about the causes and maintenance of migraines. This will enable them to understand their family members, offer them support, and help them implement preventative measures. Reading a patient guide and participating in self-help groups can be very helpful in this regard. Online social communities like www.headbook.me
What does the future hold?
Migraine is the subject of intensive international research. In recent years, it has become better understood that migraine is a very severe neurological disorder. While it is not immediately fatal, the pain, disability, and complications can still be life-threatening. The enormous societal impact of migraine also needs to be reduced. Therefore, new research strategies and efforts are underway in many areas. These are leading to a better understanding of the causes of migraine. New therapies are also on the horizon. Current research focuses, among other things, on monoclonal antibodies—immunologically active proteins that stop the inflammation associated with migraine. The so-called CGRP, an inflammatory protein, plays a central role in this process. Antibodies against CGRP are currently being developed and tested in numerous studies. Should the results be positive, these antibodies could be used in the future as a kind of passive immunization against migraine.





{kind=link}
An interesting report, especially if, like me, you have been suffering from migraines or tension headaches for 30 years and have been increasingly restricted in your everyday and professional life with the feeling that you were not allowed to reveal it. Luckily, thanks to my husband's care, I was able to reduce my working hours so that I could still combine the headache attacks and work. At work (social work) I couldn't expect any consideration for my headache attacks. The doctors only prescribed me painkillers and hormones. It was only a course at the adult education center - led by a nutritionist - that gave me the information that gradually contributed to an improvement - changing my diet, avoiding coffee and tea, reducing sugar, etc., no painkillers, exercising regularly... - and now after the menopause The bi-monthly headache attacks have almost stopped, but I am now worried about loss of vision, which is probably caused by the migraine aura. The appointment with the neurologist is still pending.
Another informative, very well described article for everyone affected and interested.
For reflection and application,
thank you Biewald Olaf