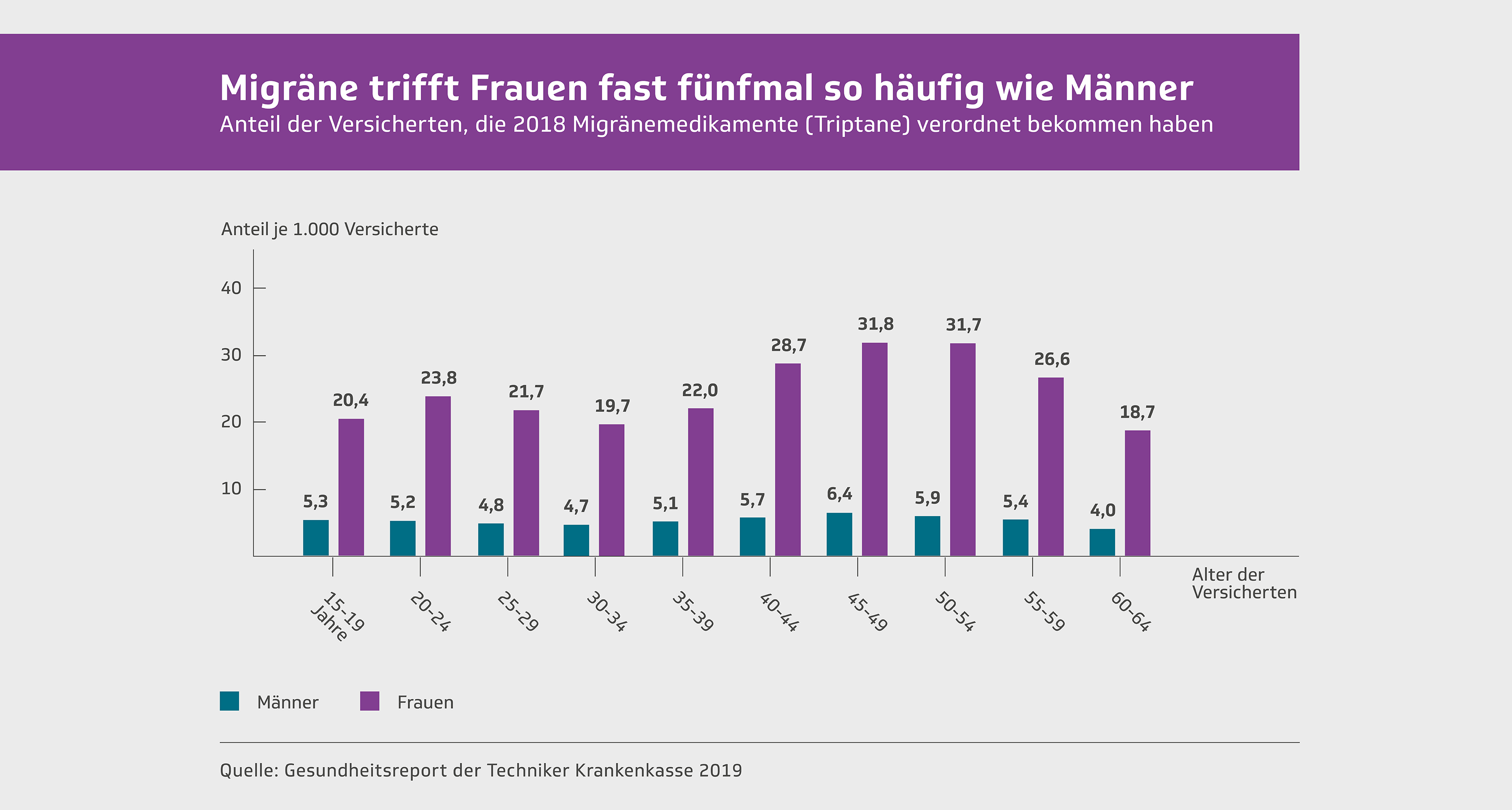


Migraines appear two to three times more in women than in men. Migraine is the most common cause of disabilities in women between the ages of 15 and 49. It has much clearer effects on women's professional career than that of men. No other disease is responsible for more lost healthy years of life in women during the active professional years. Migraines are not only more common in women, but also the seizures are heavier. They last longer, the accompanying symptoms are stronger. And they respond less well to the therapy. Many aspects in the life of women must be observed in the treatment of migraines.
The so -called menstrual migraine
The concept of menstrual migraines can be found in many publications on headache. He is used so naturally that hardly anyone has questioned him for many years. Sometimes it was even believed that the migraines are always related to menstruation. Migraines were seen as a female disease .
However, research results have shown that the combination between female hormones, menstruation, pregnancy, menopause, antibabub pill and migraines must be relativized as a matter of course.
Migraine attacks that run exclusively during menstruation are extremely rare . After a detailed survey, those affected almost always remember that they suffer not only during menstruation of migraine attacks, but also at other times in the cycle.
The concept of a menstrual migraine would only make sense if one would describe migraine attacks that occur exclusively in connection with menstruation. If you calculate the three days before and after menstruation, it can be seen that a maximum of one of 20 women who meet the criteria of migraines belongs to this group. The concept of menstrual migraines is therefore only used for a small part of the patients concerned.
Likewise, a connection with the so -called premenstrual syndrome has not yet been scientifically proven. This syndrome, characterized by abdominal pain, weakness and other psychovegetative symptoms, is about two to three days before menstruation.
Migraine attacks in a time connection with menstruation do not differ from other migraine attacks, even if a menstrual migraine is often understood to mean a particularly heavy and long -lasting attack that is associated with very severe nausea and vomiting. However, any form of migraines with or without aura can occur during menstruation. If the menstruation is actually a trigger factor, the migraine attack is usually triggered two days before menstruation.
In the patients in whom migraine attacks occur exclusively during menstruation, there is often a fixed time ratio between the attacks and menstruation. However, this time relationship can be loose in other women and the migraine attack can occur at different time intervals for menstruation.
Connection between menstruation and migraines
are triggered in connection with menstruation by dropping the estrogen and progesterone level Accordingly, the waste of the plasma -igradiol level can be held responsible for triggering the migraine attack. the absolute hormone levels do not seem to be important. An effect of the hormone on the vessels is assumed as a possible cause of the headache triggering during the estradiol waste, whereby a vascular extension was suspected due to the lower hormone concentration. So far, further analyzes of the hormone concentrations have not shown a uniform opinion on the importance of the various hormones for the triggering of the migraine attacks. Neither the follicle -stimulating hormone (FSH nor the luteinizing hormone (LH differ between patients who suffer from a menstrual migraine and healthy controls.
Treatment of menstrual migraines
Due to the time connection with menstruation, it was obvious to use hormonal therapy methods. In the past, the administration of estrogen was recommended three to 10 days before menstruation. However, it turned out that the beginning of the migraine attack is only postponed until the natural hormone drop occurs in turn.
The use of hormone plasters that release estrogens over the skin has also proven to be effective in controlled studies. The same applies to the administration of estrogens in tablet form.
Pregnancy and migraines
Mutual influence
The migraine is of particular importance for the following questions for the intended or existing pregnancy:
- How is a migraine treated during pregnancy?
- Which drugs are indicated or contraindicated?
- Is pregnancy threatened by migraine disease?
What effects can pregnancy have on the course of the migraine attack?
Fortunately, it can be seen that a very favorable influence on the course of the migraine through pregnancy can be observed. In fact, there is hardly a better prophylactic measure.
Epidemiological studies know that almost 70% of the patients concerned have a significant improvement or even a complete absence of the migraine attacks during pregnancy. The effect on the course of the migraine is particularly evident in the last two thirds of the pregnancy. It has not yet been clarified whether the positive effect is gradually subsided with repeated pregnancies on the migraines.
Only in a small part of the patients can a constant course or even a deterioration in migraines during pregnancy. This seems to apply in particular to patients suffering from a migraine with aura. If migraine attacks occur for the first time during pregnancy, it is mainly a migraine with aura. However, this is only the case with a minority of those affected; According to a French study, 13% of the patients examined. After childbirth, about half of the patients find a re -occurrence of headaches in the first week, mainly from the tension type, but also migraine attacks.
Improvement of the course of the migraine
The cause of the sometimes spectacular improvement during pregnancy has so far been completely open. However, various hypotheses are discussed:
- On the one hand, it is assumed that the constantly increased concentrations of estrogen and progesterone cause improvement during pregnancy.
- Other explanations assume that a changed serotonin metabolism during pregnancy and an increased concentration of endogenous opioids, i.e. opiate -like substances made by the body, are responsible for improvement.
- In any case, the changed lifestyle during pregnancy seems to be of crucial importance. Pregnant women eat more consciously, have a regular sleep-wake cycle, avoid alcohol and nicotine, try to live less stress and are less stressed in the work process. There is a pregnancy-related control of trigger factors and accordingly fewer migraine attacks are triggered. However, there are no empirical studies that confirm this hypothesis.
Migraine prevention during pregnancy
In general, drug therapy should be avoided during pregnancy if at all possible. Of course, this particularly applies to prophylactic measures where medication must be taken daily. The migraine prophylactics that have proven to be particularly effective are contraindicated during pregnancy. This applies to beta-receptor blockers, flunarizine, serotonin antagonists, tricyclic antidepressants and especially antiepileptic drugs. This is particularly important if a pregnancy is planned or even suspected. Since young women in particular use such medications for severe migraines, they must be made aware of the need for adequate contraception.
To prevent migraine attacks during pregnancy, as usual, behavioral measures such as:
- relaxation exercises and
- Getting to know and avoiding trigger factors.
- If migraines are severe during pregnancy, especially migraines with aura, administration of magnesium for migraine prophylaxis can first be considered. The effect of magnesium on the course of migraines has generally been shown to be small in clinical studies, but in individual cases a significant effect can be achieved.
- Propranolol is used to treat arterial high blood pressure during pregnancy . There is no evidence of a fetal disorder. Nevertheless, the use of propranolol during pregnancy to prevent migraines should be carried out very cautiously and should only be considered as a last resort.
Treatment of migraine attack during pregnancy
There is very little literature on the effectiveness and tolerability of medications for the treatment of migraine attacks during pregnancy. The same applies to the effects of medicinal migraine therapy on childbirth and breastfeeding.
Non-steroidal anti-inflammatory drugs such as ibuprofen or diclofenac should only be used in exceptional cases and only in the 2nd trimester of pregnancy.
Paracetamol has long been considered the analgesic of first choice in pregnancy, but is increasingly associated with later health problems in the child (increased risk of bronchial asthma, disturbance of the child's psychomotor development or cryptorchidism in boys). However, the data currently does not allow a final assessment of the risks. In view of the low effect of paracetamol on migraines, the use of the substance during pregnancy is currently no longer recommended (see below).
not during pregnancy . On the one hand, there is insufficient experience, and on the other hand, it has not been proven that they end migraine attacks more effectively than the above-mentioned substances that have been used for many decades. Particular care must be taken to ensure that nonsteroidal anti-inflammatory drugs are not used continuously. Particularly during the last trimester of pregnancy, there is a risk of prolongation of the pregnancy, an increased risk of preeclampsia, an increased risk of bleeding for mother and child and an increased risk of persistent pulmonary hypertension in the child.
Warning about paracetamol during pregnancy
New studies describe a possible link between exposure to paracetamol before birth and increased risk of asthma, other respiratory diseases and impaired testicular development.
Paracetamol was previously considered the safest painkiller during pregnancy. Based on previous data, safety appeared to be beyond doubt. Pregnant women were recommended to take this painkiller almost without hesitation if they had pain during pregnancy. However, based on recent studies, careful rethinking of this recommendation is necessary. New studies describe a possible link between exposure to paracetamol before birth and increased risk of asthma, other respiratory diseases and impaired testicular development. Disturbances in the child's psychomotor development are also discussed. Contrary to previous recommendations, it is therefore not recommended to take paracetamol in mono- and especially combination preparations if you are pregnant or are already pregnant.
Until the exact connection is clarified, the principle must apply: In case of doubt, for the unborn life and against taking paracetamol, especially in combination with other painkillers.
Short benefits and long -term lifelong risks are no longer in a balanced relationship with possible or existing pregnancy due to the new data.
The use of paracetamol by the pregnant woman and the unborn child's exposure to the drug appear to lead to a significantly increased risk of developing asthma and respiratory diseases in children and possible infertility in boys. In recent years there has been a significant increase in the frequency of asthma globally. Paracetamol is one of the most commonly used medicines in Germany. Paracetamol can lead to a reduction in glutathione in the lungs. Glutathione is believed to play an important role in the development of asthma.
According to new study results, the well-founded suspicion of a significantly increased risk of developing the positional anomaly of the testicle in boys (cryptorchidism) is particularly worrying. For those affected, this can later lead to reduced fertility and an increased risk of developing malignant testicular tumors. Sperm count and sperm vitality in later life may be reduced. The combined use of two painkillers in pregnant women was associated with a 7-fold increased rate of cryptorchidism in newborn boys. It is suspected that the effects of one 500 mg tablet of paracetamol could be more harmful to the unborn child than the ten most common environmental pollutants. The studies were criticized because a causal connection had not yet been definitively proven.
Previously, paracetamol has been considered a safe, harmless, tolerable and inexpensive pain reliever in therapeutic doses. The risk that irreversible liver cell damage to liver failure can be triggered with overdosing over 150 mg per kg body weight, has already led to a limitation of the pack size as part of self -medication. The new studies justified a significant rethink for the use of possible, planned or existing pregnancy.
In general, you should avoid taking painkillers during pregnancy and breastfeeding. In individual cases, if the pain is particularly severe, acute medication can be considered after medical advice. However, it must be taken into account that so-called simple painkillers such as paracetamol only have a weak and short effect on the severe attack of pain, but at the same time can cause lasting lifelong risks for the unborn child.
Contrary to previous recommendations, it is therefore not recommended to take paracetamol in mono- and especially combination preparations if you are pregnant or are already pregnant.
Triptane
The company pregnancy register has not yet shown a significantly increased risk of malformations when using sumatriptan in the first trimester of over 1000 pregnancies.
For the other triptans, there is insufficient data to assess the safety in pregnancy. not be used during pregnancy
Ergot alkaloids such as ergotamine tartrate and dihydroergotamine are strictly contraindicated. The substances have a uterotonic effect during pregnancy. In addition, ergotamine has a toxic effect on the embryo.
Treatment of migraine attack during breastfeeding
Painkiller
Ibuprofen is the analgesic of choice during breastfeeding. When taken sporadically, it only passes into breast milk in very small amounts and is even approved for the treatment of newborns.
Triptane
Triptans pass into breast milk. For sumatriptan, the specialist information recommends a 12-hour break from breastfeeding after taking it, and 24 hours for all other triptans.
Behavior when you want to get pregnant
- In the first 14 days after the first day of the last menstrual period (assuming a regular 28-day cycle (!)) it can be assumed that there is no pregnancy.
- With a regular cycle, ovulation occurs approximately 14 days BEFORE menstruation.
- Six days after ovulation, the fertilized egg implants in the uterus and thus the first contact between “mother and child”.
- Medical treatment of migraine attacks is possible for a period of the first three weeks after the first day of the last menstruation without endangering the fruit.
- Existing pregnancy can be used with newer pregnancy tests from 6-10. The day after ovulation, there is a few "unsafe" days about three weeks after menstruation, in which one recommends carrying out a pregnancy test before taking acute medication.
Birth control pills and migraines
In the case of persistent migraine attacks that are difficult to treat, birth control pills are often blamed for triggering the attacks. Empirical testing of a connection between birth control pills and migraines, on the other hand, does not show a clear connection: some studies speak of an actually increased occurrence of migraine attacks, although this is said to be the case in 18-50% of affected patients, depending on the study. In other studies, therapy with the contraceptive pill actually shows an improvement in migraines in up to 35% of patients. In so-called double-blind studies, however, no significant difference was found between groups of patients who were treated with the contraceptive pill or placebo.
All in all, it appears that there is no definitive connection between the birth control pill and migraines.
The treatment of migraines does not differ if you are taking a contraceptive pill or not. Birth control pills and migraine medications are also not known to affect each other. When carrying out migraine therapy, the same guidelines apply as usual.
It is only advisable to try skipping the contraceptive pill for migraines, which occur rarely and do not respond to drug therapy. The patient should then be recommended another method of contraception.
Because of the increased risk of arterial or venous cerebral thrombosis and cerebral hemorrhage, a neurological examination should be carried out as soon as possible if neurological disorders suddenly occur.
This also applies when unknown headache attacks occur. For this reason, patients who take birth control pills in particular should be monitored at closer intervals to see how the disease is progressing. Smoking should be strictly avoided. This is particularly true due to the possible increased risk of stroke with migraine disease. Overall, however, this risk of an increased frequency of strokes with migraine is extremely low. Migraine is therefore in no way a contraindication to the use of oral contraceptives. Menopause and older age
It is often the opinion that migraines gradually “burn out” as we get older, i.e. their frequency and intensity decrease. However, studies that deal with this complex of questions show that in more than 50% of those affected there is no change in the previous course of migraines . Around 47% of patients even experience a deterioration.
The increased frequency of migraines in women compared to men also persists in old age. Hormone therapies in old age cannot influence migraines. Accordingly, in this age group, migraine therapy should be carried out as usual.
However, beyond the age of 75 or 80, a change appears to occur. In fact, there are hardly any patients in the specialized migraine outpatient clinics who are older than 80 years and complain about migraine attacks.





{kind=link}
Leave a comment