
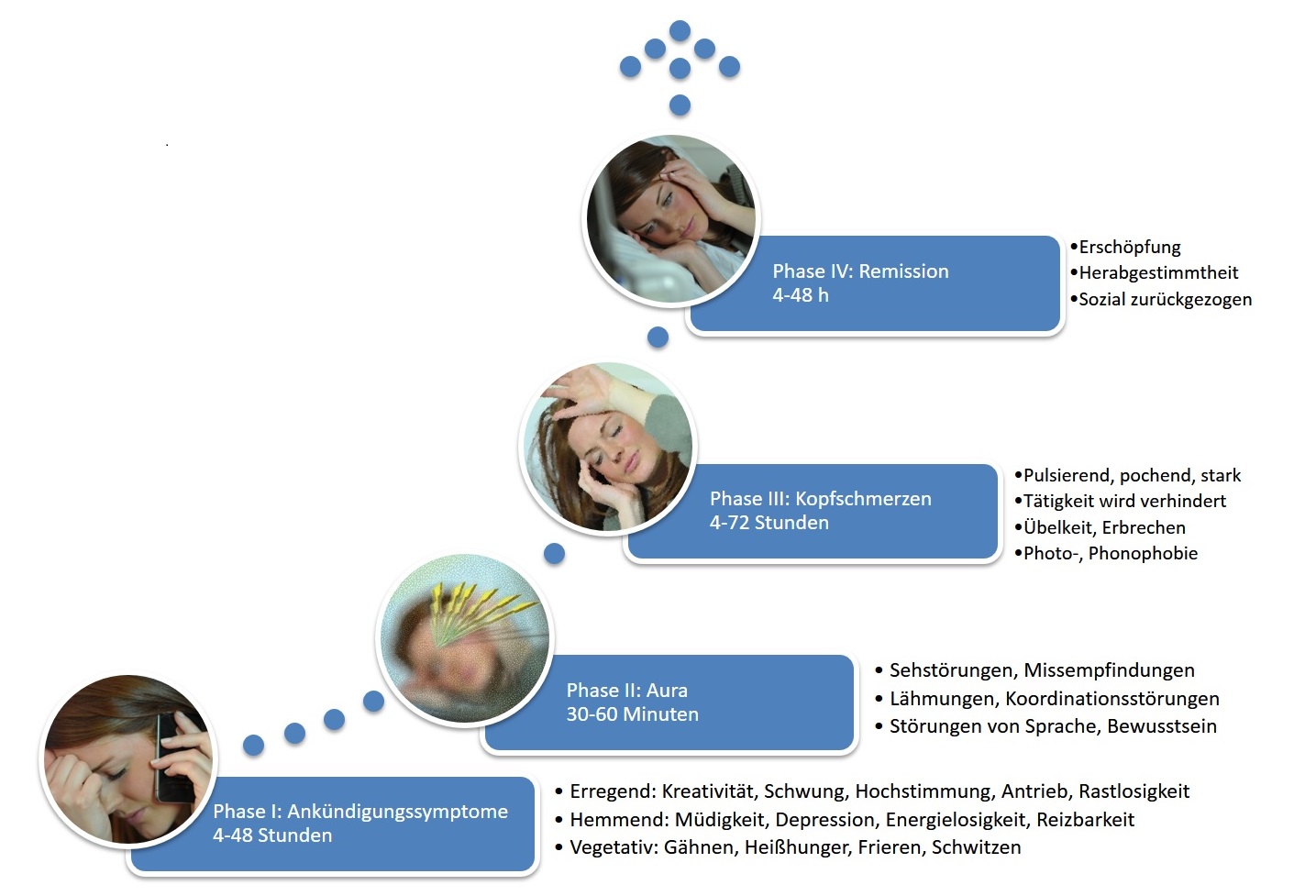


One of the peculiarities of migraine attacks, from the sufferer's perspective, is that they always strike at the most inconvenient times. While the individual course of a migraine is unpredictable, it does follow certain patterns: a migraine is over within 72 hours at the latest. This biological constant is also reflected in the diagnostic criteria for migraine (the International Headache Society's (IHS) headache classification): a key criterion for migraine is an untreated duration of headache attacks of 4 to 72 hours.
Unfortunately, there is an exception to this rule: status migrainosus. This term refers to migraine attacks that last longer than 72 hours for whatever reason. Status migrainosus is listed by the IHS as a migraine complication.
If patients are asked whether they have ever suffered from such long migraine attacks, the majority will confirm this. For most sufferers, it will have been an exception. However, for some, these long, debilitating, and exhausting migraine attacks are the norm. Three scenarios are particularly typical:
- Menstrual-associated status migrainosus:
A common trigger for prolonged migraine attacks is the hormonal changes at the time of menstruation. After two to three days of migraine, which can be treated more or less effectively, the headaches subside. The woman seems to have overcome the attack, only to experience, after a short break of a few hours, the return of the migraine on the other side of her head, where it rages for just as long again. - Therapy-resistant migraine attack:
Many patients actually have access to effective medication for migraines, which they can usually rely on even during severe attacks. However, there are also attacks where this otherwise effective approach fails. The first dose of triptans brings no relief whatsoever, and a second dose, taken against one's better judgment, also has no effect. One resorts to painkillers, which have never really helped anyway, and sure enough, they don't help now either. All that's left is the bed and the hope that the migraine will eventually subside on its own. But this particular attack doesn't disappear after three days. - Status migrainosus due to medication overuse:
Here, the situation is initially completely reversed. The migraine can be effectively stopped with medication, usually a triptan, but only seemingly. As the triptan level drops, the migraine returns after 12 to 24 hours, a phenomenon known as a rebound headache. Inevitably, the triptan is taken again (which is permissible once within 24 hours according to the dosage guidelines), and again it works: the migraine pain subsides. But this time, the effect doesn't last as long. The following hours and days are then characterized by a fluctuating migraine. While repeated doses of painkillers and triptans can achieve temporary relief, the effect becomes progressively weaker and shorter-lasting. Complete pain relief is no longer achieved; only the peak pain episodes can be alleviated. The pain pattern becomes increasingly unclear, pain-free periods steadily decrease, the pain often strikes in the early morning, waking the person from sleep, resistance to migraines diminishes, mood deteriorates, the pain increases irritability, tension, and lethargy, and motivation and performance are progressively reduced. Eventually, the moment arrives when nothing helps anymore. And once again, all that remains is the bed and the hope that the migraine will eventually subside on its own. But even this attack doesn't disappear after three days; exhaustion, hopelessness, and resignation increase.
Therapy of status migraenosus
Depending on the type of status migrainosus, different treatment options are available.
prevention
Menstrual-associated status migrainosus is a predictable event, making it amenable to targeted preventive measures. If migraine with aura is not present, the hormonal drop that triggers this migraine attack can be counteracted with hormone therapy. This is simplest for women who are already using hormonal contraception with a combined estrogen-progestin preparation. Instead of pausing the pill for seven days after every three weeks, it can be taken continuously in a 21-day cycle (3 x 21 days) or a 21-day cycle (6 x 21 days). This means that menstruation, and therefore menstrual-associated migraine, only occurs every three or six months, respectively. An alternative approach without hormones involves taking a long-acting triptan such as naratriptan or frovatriptan, or the long-acting pain reliever naproxen, preventively twice a day for one week. Treatment begins two days before the expected onset of menstrual-associated status migrainosus. This approach can only be used if there are few headaches requiring treatment during the remainder of the cycle, thus minimizing the risk of developing medication-overuse headache.
If status migrainosus occurs independently of the menstrual cycle, all standard pharmacological and non-pharmacological options for migraine prevention are generally suitable. The goal of migraine prevention is not only to reduce the frequency and intensity of migraines, but also, and especially, to reduce the duration of attacks.
Another option for preventing status migrainosus is the primary prevention of recurring headaches. Particularly when triptans are administered alone, recurring headaches occur in 25 to 50% of attacks, depending on the specific drug. This rate can be reduced by taking the long-acting anti-inflammatory analgesic naproxen concurrently with the relatively short-acting triptan at the onset of the migraine attack.
Acute treatment
Preventive measures come too late once status migrainosus has already set in. Experience shows that taking triptans and/or painkillers during status migrainosus becomes less effective and shorter-lasting with each passing day, and instead of ending the migraine, the medications only prolong the attack. Therefore, the general recommendation is to avoid painkillers and triptans from the fourth day of a migraine onward. Even if it seems unlikely, the quickest way out of status migrainosus is to avoid taking any acute medications such as painkillers or triptans that were taken before. Anti-nausea medications are more effective. The over-the-counter medication dimenhydrinate, known under the brand name Vomex® A , among others, now offers the advantage over metoclopramide (MCP) of an additional, mildly sedating effect. This so-called sedative effect can also be achieved with weak neuroleptics such as promethazine or melperone, and with tricyclic antidepressants such as amitriptyline, doxepin, or trimipramine. In exceptional cases, a tranquilizer such as diazepam can also be considered; however, these should be used very sparingly due to the potential for dependence. All of these substances require a prescription. The ultimate goal is to enable the affected person to keep the pain out of their conscious awareness through a pain-distancing effect, without having to take a painkiller or a triptan. Fatigue and bed rest must be accepted as part of the process. Understandably, the ability to work is not achieved during this phase. Taking triptans or painkillers in this situation with the aim of functioning quickly leads to medication overuse and is not a sustainable solution.
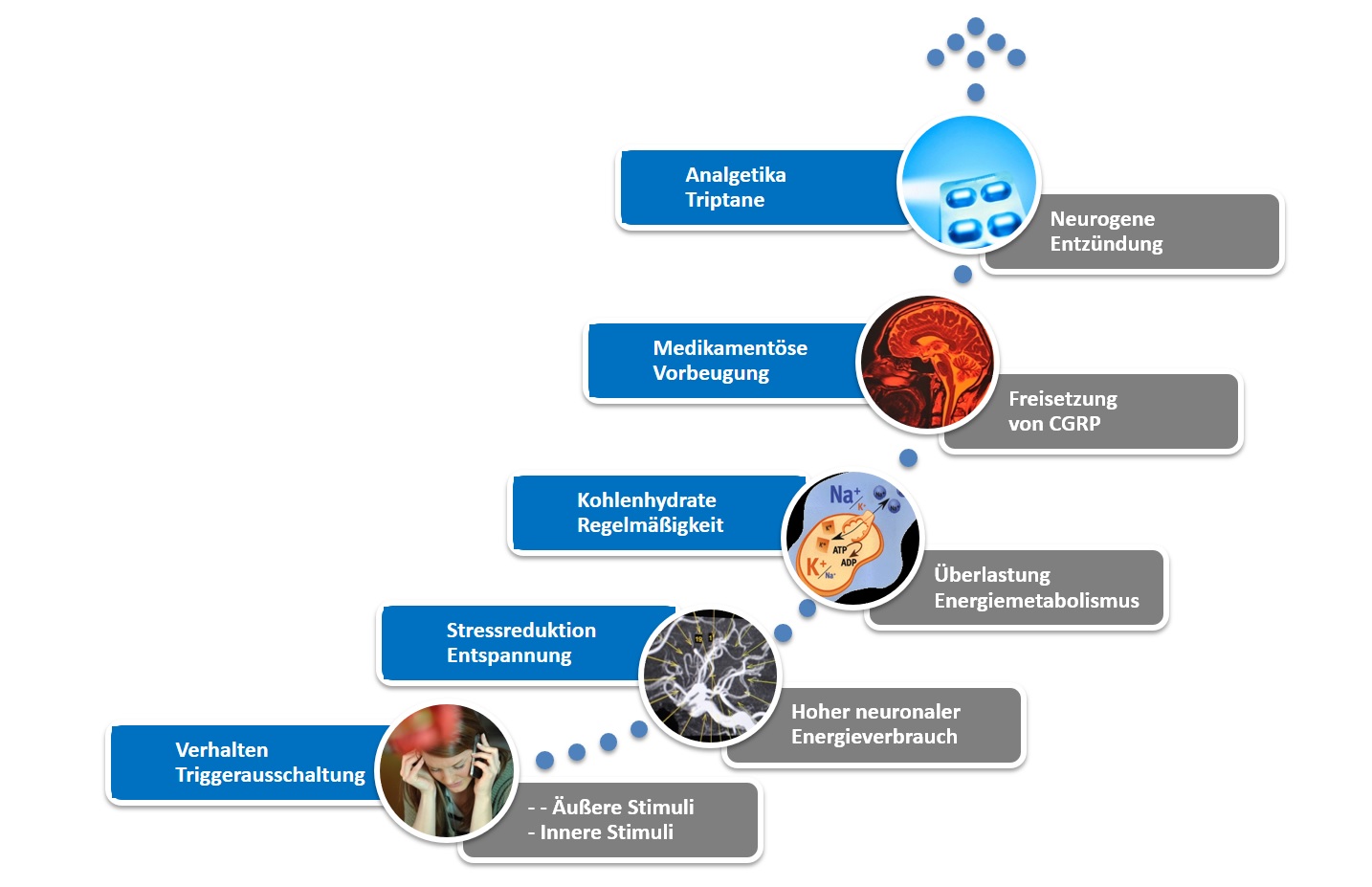
Another therapeutic approach is to block the inflammation of the blood vessels in the meninges that underlies migraine pain by administering prednisolone or other cortisone preparations, thereby eliminating the biological basis of the pain. In emergency situations, the cortisone is usually administered intravenously, which offers the advantage of a relatively rapid onset of action while bypassing absorption in the gastrointestinal tract. However, for many sufferers, self-administration of 50 to 100 mg of prednisolone as a tablet also leads to improvement within an acceptable timeframe. If necessary, the morning dose can be repeated for two or three days until the inflammation subsides completely. Prednisolone is also available only by prescription.
However, individual consultation and examination are always necessary. The specific course and pattern of seizures must be analyzed. Preventive measures must be optimized. These include behavior and, if necessary, medication. The latter can usually only be effective and well-tolerated if used correctly. Here, too, knowledge is the best medicine.
Dr. Katja Heinze-Kuhn, Dr. Axel Heinze, Prof. Dr. Hartmut Göbel,
Neurological-Behavioral Medicine Pain Clinic Kiel





{kind=link}
As a sufferer, I couldn't have described the chronic migraines better during menstruation, but also when medication is overused. Word for word, that's how it happens for me too. The only thing that surprises me is that when I describe my pain attacks in exactly the same way to neurologists and pain therapists, I always get the impression that they can't do anything with it. I still have the feeling that my pain experiences are different than those of other sufferers.
I also think it's a shame that you have to read about many therapy attempts yourself (including those described in this article) and then convince your doctor to give them a try. Actually, in my opinion it should be the other way around.
I have chronic migraines that currently last up to 20 days a month and usually take significantly more than 10 triptans.
Hello,
I have almost only had aura without headaches for a year now, with speech problems, weakness on one side from head to toe that constantly changes sides, basically jumping back and forth. Also pins and needles, mainly on the face. For me these auras regularly last at least 1 week! Luckily everything went away again. I also had to jump back and forth for three weeks in a row with severe pain. I usually have cap-like pressure on my head at the end of the week. I had an MRI twice, and the cerebrospinal fluid and long-term EEG are also OK so far. I just really wanted to get rid of the fact that, like mine, there are so-called prolonged auras and that such a long aura is not immediately a migranous infarction like in the diagram. I would be very happy to receive comments from a technical perspective. I am very desperate and no longer able to work.
I recently had a similarly bad experience of recurring migraines within 5 days. I took 25 mg sumatriptan (suppositories) a total of 4 times, whatever helped. I otherwise very, very rarely take triptans and often get my migraine under control with 10-minute contrast showers.
Question: During cataract surgery I was given propofol as sedation on both eyes and then I always got severe migraines on the following day or even the day after, most recently the one described above.
Could this be the effects of propofol?
Greetings
Anna Schmitz
I was in the pain clinic in December 2015 and am infinitely grateful to all the staff and to Professor Göbel that I have fewer attacks and am able to endure the tension headaches even without painkillers.
They often disappear within a few hours. This is a wonderful experience after years of taking painkillers. The migraines currently only come 2-3 times a month, but sometimes 3-4 days. I usually don't take any painkillers on the first day and sometimes none on the last day either, so my medication days have been significantly reduced. Many thanks to Prof. Göbel for his support and empathy. My 11-hour working days (including 4 hours of driving time) on the Baltic Sea are no longer quite as hard for me; I can still manage it twice a week.
Thank you, thank you, thank you, I hope it stays that way!
LG Elena
I read your report with interest, I too have been suffering from hormonal migraines for around 20 years and now only after many and long experiments, for example. Currently only Vomex because it makes you so tired. I also take hormone gel about 4 days before my period starts, which I then take for a total of about 10 days. Would it perhaps help to take additional prednisolone or is that not recommended? LG
I was in the pain clinic last month for, among other things, an almost daily medication overuse headache. In the clinic I had a violent attack, which I survived without painkillers but with Vomex and Melperon. I have just completed the 4-week medication break and so far have only had the attack in the clinic and 2 days at home, the remaining days pain-free, without triptans etc. Thank you for the Kiel Pain Clinic, I look to the future with confidence !!
Thanks for the information.
For me, acute treatment for status migraenosus helps: Vomex, but diazepam is better. Don't go to work, stay in bed, darken.
Take as prophylaxis: gabapentin, topiramate and venlalexin.
Had about 20 attacks in January, I'm currently at about 8.
Greetings Alex Rochmann
Thank you for this interesting article. I also have recurring attacks every day (sometimes for more than 10 days in a row), but the triptan helps me within 2-3 hours and the migraine doesn't come back until the next morning. I'm fit for the day and have no pain. Is this also a medication-dependent migraine even though the medication banishes the pain for about 20 hours?